☠️ Approach to Ischemic...

Highlights
- ☠️ Approach to Ischemic Limb Syndromes ☠️
You're in the ICU examining a patient & find a patient with purple discoloration of an extremity concerning for limb ischemia
But the patient has distal pulses!
What's going on? 🧐
Take a journey with me & @OmarosisFugax!
 (View Tweet)
(View Tweet)
- First, when should we be concerned about an Ischemic Limb Syndrome?
Let's keep it simple:
⛳️ Extremity pain (if patient can report)
+
⛳️ Skin changes (eg pallor, purpuric → bullous lesions, blue-discoloration, necrotic changes) (View Tweet)
- There are 2 key questions when assessing your patient with an Ischemic Limb Syndrome:
- Pulse/Arterial Doppler? 🤏
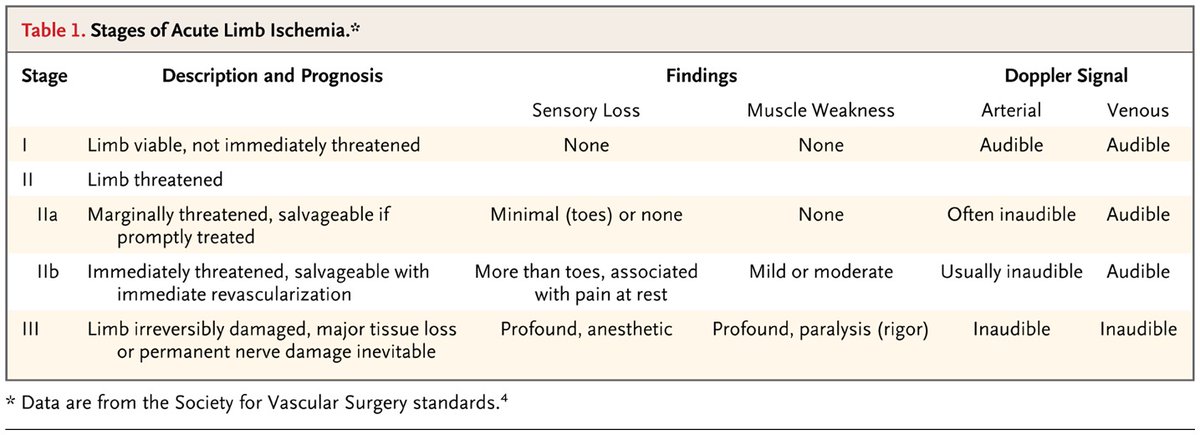
If Pulse/Doppler are (–), you're likely dealing with Acute Limb Ischemia (ALI). Remember the P's:
- Pain, Paresthesia, Paralysis
- Pallor, Poikilothermia
 (View Tweet)
(View Tweet)
- If Pulse/Doppler are (+), time to redirect your attention away from acute arterial occlusion toward the:
🔵 Venous system
🔵 Microscopic vasculature (ie arterioles, capillaries, venules)
To tease out which system is at play, ask yourself question #2:
2) Is there a DVT?
 (View Tweet)
(View Tweet)
- If an extensive DVT is present, you may be dealing with ischemia due to compromise of the large venous vessels, leading to a non-gangrenous, reversible condition:
🔵 Phlegmasia Cerulea Dolens
- Patients with Phlegmasia classically have a painful, blue, swollen leg
 (View Tweet)
(View Tweet)
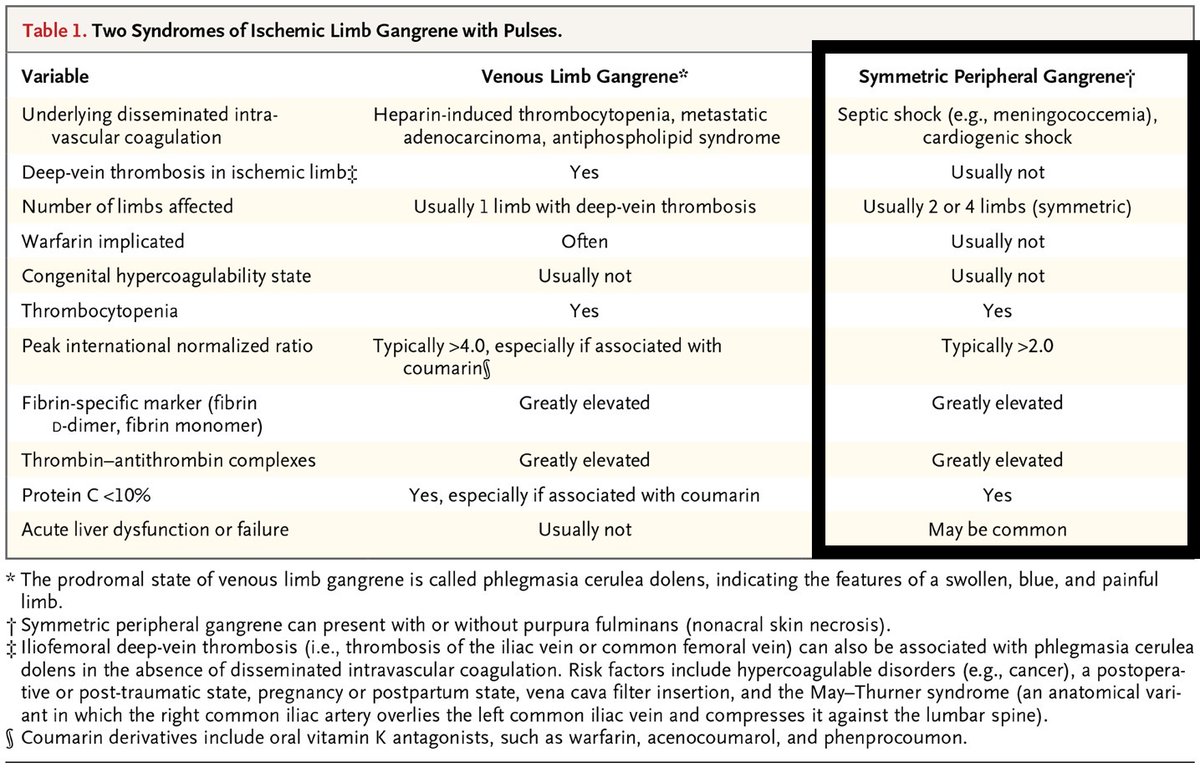
- If untreated, Phlegmasia may irreversibly progress to Venous Limb Gangrene ☠️
Some quick points on DVT-associated limb ischemia:
🔵 Classically, symptoms are unilateral & ipsilateral to the DVT
 (View Tweet)
(View Tweet)
- 🔵 If discovered, you should also consider the driver of DVT formation, because DIC is often at play. Common drivers include:
- 💊 Warfarin use must also be considered, as warfarin is often implicated in Venous Limb Gangrene
💊 Of note, "Warfarin skin necrosis" is a distinct entity involving primarily the skin, whereas Venous Limb Gangrene often involves deeper tissues (ie ↑ amputation risk)
 (View Tweet)
(View Tweet)
- Back to our schema!
🔍 If the patient does not have a DVT, your focus is now on microscopic vascular occlusion 🔍
Before diving into our endpoint diagnoses, let's review 2 related, "can't miss," DIC-related syndromes:
🔴 Symmetric Peripheral Gangrene
🔴 Purpura Fulminans
 (View Tweet)
(View Tweet)
- Symmetric Peripheral Gangrene (SPG) & Purpura Fulminans (PF) are typically seen in shock patients with ↓ platelets & coagulopathy
🔴 Symmetric, distal ("acral") necrosis = Symmetric Peripheral Gangrene
🔴 Non-acral, multicentric, extensive necrosis = Purpura Fulminans

 (View Tweet)
(View Tweet)
- ⚪ Pearl: preceding shock liver is seen in ~90% of patients who develop Symmetric Peripheral Gangrene!
- Skin findings usually begin 2-5 days after the initial transaminase elevation
- This time period may reflect the time needed for critical depletion of protein C levels
 (View Tweet)
(View Tweet)
- After considering SPG & PF, etiologies of "DVT-negative" Ischemic Limb Syndromes can be clustered:
"What can plug a microscopic vessel?"
👇
- Clots
- Emboli
- Proteins
- Inflammation
- Infections
- Crystals
Let's review a few endpoint diagnoses...
 (View Tweet)
(View Tweet)
- Emboli 💦
- SEPTIC: while the Osler nodes of infective endocarditis (IE) are pathognomonic, eponymic findings are actually less common
⚪ Of the <10% of IE patients with skin findings, purpura is most common & seen in ~8%! Extensive necrosis may be seen!
 (View Tweet)
(View Tweet)
- Proteins 🟢
- TYPE 1 CRYO: skin findings are seen in ~70-85% due to monoclonal cryoglobulin precipitation → purpura, livedo reticularis → ulceration
 (View Tweet)
(View Tweet)
-
- CRYOFIBRINOGENEMIA: cold-induced fibrin/fibrinogen precipitation → presentation similar to Type 1 cryo
- PARAPROTEINEMIAS: purpura can be seen in myeloma & Waldenstrom's due to non-cryoglobulinemic Ig deposits
 (View Tweet)
(View Tweet)
- Inflammation 🔥
- A number of SMALL/MEDIUM-vessel vasculitides can occlude the microvasculature, & isolated skin involvement can be seen in cutaneous small-vessel vasculitis
- THROMBOANGIITIS OBLITERANS: think young smokers with digital ulceration/gangrene
 (View Tweet)
(View Tweet)
- Some final helpful notes 📚
⚪ The purpura in these etiologies are frequently described as "retiform." This refers to a branched appearance of the dark red/purple purpuric lesions & signifies complete occlusion of the skin's microscopic vessels
 (View Tweet)
(View Tweet)
- ⚪ Livedoid vasculopathy: refers to skin biopsy showing microvascular thrombosis, endothelial proliferation, & subintimal hyaline degeneration → "livedoid changes" → ulceration. This is often secondary to pro-thrombotic disorders & rheumatic diseases!
 (View Tweet)
(View Tweet)
- ⚪ Since each endpoint Dx can manifest with "retiform" purpura (potentially progressing to ulceration/necrosis), how can you make diagnostic progress? Consider the following:
- Time course
- Distribution (eg acral vs. non-acral)
- Extra-dermatologic involvement
 (View Tweet)
(View Tweet)
- ⚪ Finally, consider mimickers!
🎭 Necrotizing skin/soft tissue infections (SSTIs)
🎭 Neutrophilic dermatoses
🎭 Trauma-related etiologies
(Note: there is some overlapping pathophys w/ the buckets of the "DVT-negative" list, but we've included this separately for simplicity.)
 (View Tweet)
(View Tweet)
- Before our 🏁 Takeaways 🏁 please give @OmarosisFugax a follow.
This schema & thread were co-created with Omar via numerous iterations behind-the-scenes. It simply wouldn't be the same w/o him & I'm so glad we collaborated. (View Tweet)
- 🏁 Takeaways
- If concern for an Ischemic Limb Syndrome (ie extremity pain + skin changes), first look for Pulse/Doppler signal, then consider DVT
- If pulses are (+) & there's no DVT, consider microvascular occlusion
- Prioritize SPG & PF in critically ill patients!
 (View Tweet)
(View Tweet)
- Save this schema on Glass (@GlassHealthHQ) here!
https://t.co/ONb8q4RUpd (View Tweet)
- References:
- https://t.co/pW9lCZiTFM
- https://t.co/PIEQ09uDAz
- https://t.co/c42nqgdVNS
- https://t.co/J0D0vq1gaa
- https://t.co/8uFxGAKcrZ
- https://t.co/zPZ66cEVEz
- https://t.co/b3a9PVq0yS
- https://t.co/EdfL9wTxvb (View Tweet)
- CC: @rabihmgeha @DxRxEdu @Sharminzi @AndreMansoor @rav7ks @KirtanPatolia @Rafameed @MadellenaC @Marcelaaos @AnnaFretz @ShreyaTrivediMD @AdamJBrownMD @medpedshosp @DrDanRestrepo @nsrosenberg @dereckwpaul @NazliDizman @MatthewHoMD @adil_rashidk @haematognomist @HannahRAbrams (View Tweet)
- @preardon @YaleIM_Chiefs @MarkDSiegel1 @Dr_AmerZeidan @ElizabethPrsic @tony_breu @DoctorWatto @PaulNWilliamz @Sofiacruzsolbes @RMadhavanMD @Heard_that_alex @SJMagierMD @ana_ferrigno @AnnSolimanMD @PulmCrit @AaronGoodman33 @LandsbergManual
@TheRealDSrini @DruvBhagavan
@PBlivenMD (View Tweet)

 (View Tweet)
(View Tweet)